We can’t keep saying yes.
How workforce erosion is undermining cancer care in the NHS.
“You just need to go faster, go further”.
“If we could always start with ‘Yes, we can do it”.
“It’s about the patients now”.
These were the sentiments of senior NHS England representatives at a meeting for heads of departments last October.
As I listened, I felt first like a reprimanded schoolchild, then stunned and finally angry. Faster and further might be the message a support team gives to an ultra-runner attempting a record. In the NHS, it lands differently. And ‘It’s about the patients now’ implies that somehow, it wasn’t before.
Since October 2023, I’ve been joint Head of Service for oncology at one of the largest acute trusts in England. It’s a trust full of committed, skilled, compassionate people doing everything they can for patients in increasingly impossible circumstances. It’s also a trust facing enormous financial pressures. For 2025-2026 our savings target was just under £100m, much of it coming from reducing corporate and support staff and limiting recruitment.
In my opinion, cutting support services is not just difficult, it’s counterproductive. This isn’t cost-saving. It’s cost shifting, moving from lower-paid roles to higher paid ones, and from prevention to crisis management.
We can’t simply say yes.
During the meeting I asked how we should communicate and engage colleagues who already feel stretched and unsupported, given the “further faster” and “start with yes” expectations. The responses largely didn’t address the communication challenge, instead focusing on improving efficiency and making better use of existing resources.
The argument from NHS England is that there is unwarranted variation, and that some organisations are delivering better outcomes with similar resources. That may be true. But it risks overlooking a critical point: much of the inefficiency we are being asked to address is structural, not behavioural. In systems where the foundation has been eroded, it is not realistic to expect clinicians to simply “work harder” or “say yes” their way to improvement.
Do I think we’re working as efficiently as we could be? The honest answer? No. But not for reasons within our control. We are far from efficient. And in my opinion, a large part of that inefficiency is the systematic erosion of the workforce from the bottom up.
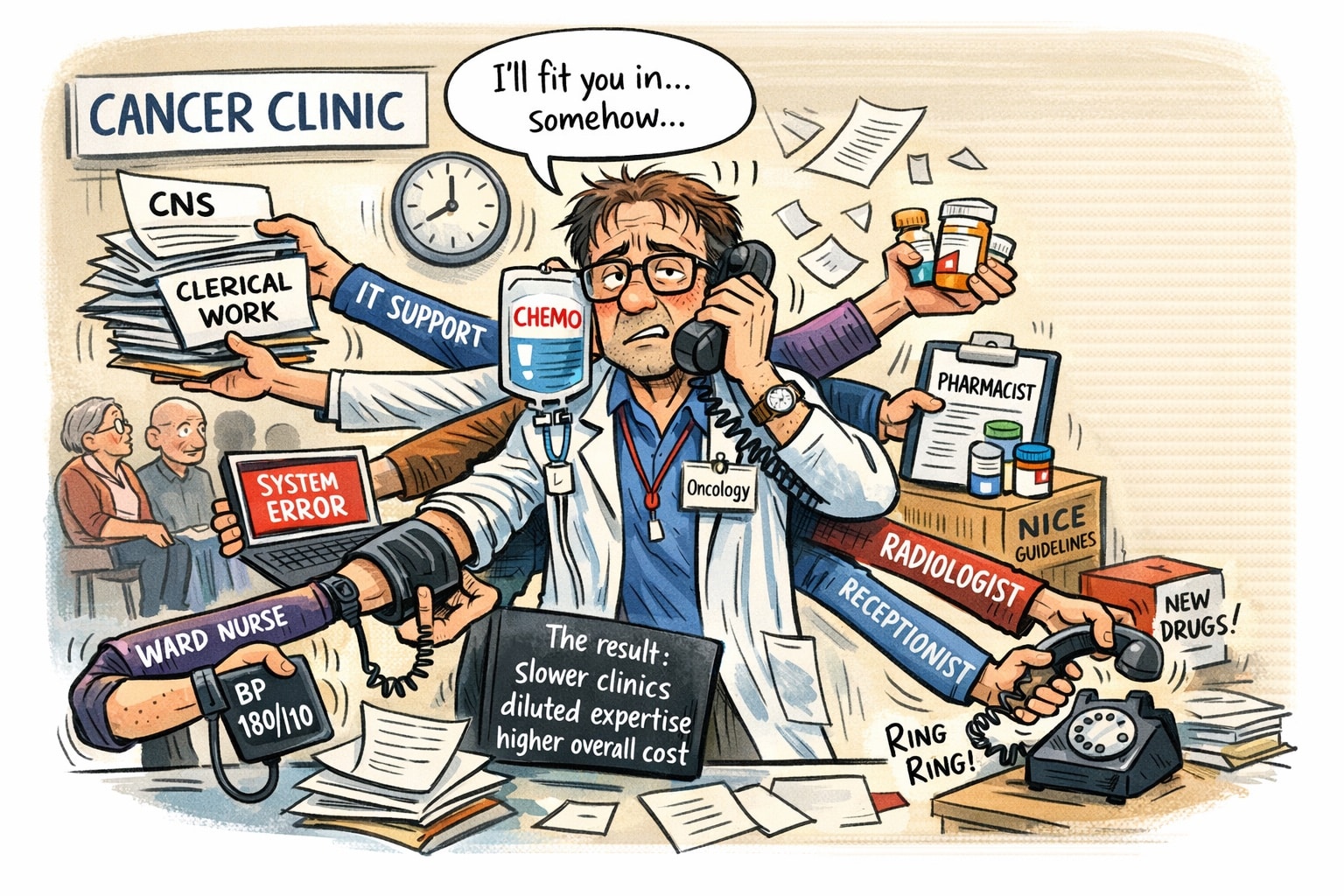
Our oncology administrative staff are the backbone of cancer care. They coordinate outpatient pathways, schedule chemotherapy, manage communication between primary and secondary care, ensure the trust is reimbursed for the clinical work performed and are often the first port of call for anxious patients and carers. They bring order to inherently complex systems and without them, much of what we do crumbles.
And they are disappearing.
Where once a single support staff member might support one or two consultants, they now support six. Experienced colleagues are overwhelmed, demoralised, off sick and increasingly considering leaving. Those who remain know they are not able to deliver the service patients deserve. And, since the work they do is essential, it’s now being undertaken by higher paid staff who deliver the workload far less efficiently.
We lack the basic digital infrastructure that might compensate. Despite widespread access to technology outside the NHS that would allow us to dictate letters in realtime, we have no effective automated systems in place. We don’t have enough typists, so typing falls to already overstretched, and more highly paid admin teams. Letters are delayed by weeks, sometimes no longer clinically relevant. This delay impacts GPs, who rely on timely correspondence to manage their patients safely and effectively. For a cancer patient, receiving outdated reassurance after disease progression is not just inefficient, it’s harmful.
Without sufficient admin staff, highly skilled clinical nurse specialists (CNSs) are doing administrative work. The government’s cancer plan states ‘Every patient will have a clinical nurse specialist or other named lead to support them through diagnosis and treatment’. At my trust we currently have just 1.4 whole time equivalent secondary breast care nurses to support around 600 patients. This equates to roughly five minutes per patient per week. That’s not a service. It’s a compromise.
Without enough CNS staff, consultants absorb nursing tasks. Patients lose access to the support they need and deserve, and doctors cannot work efficiently. As waits accumulate, the system compensates with agency staff or extra clinics, expensive fixes for problems that could be prevented by building from the bottom up.
For inpatient care, the same pattern repeats. Limited weekend imaging capacity means patients stay in hospital unnecessarily over weekends waiting for scans or interventions. Fewer phlebotomists mean more highly paid ward doctors take bloods, often late in the day after their ward rounds, delaying results and decisions. Nurses do healthcare assistant work. Doctors do nursing tasks. Everyone routinely works below their skillset.
This is not efficiency. It’s dilution of expertise. And it’s expensive. Patients stay longer, beds remain occupied, and flow through the hospital slows.
Highly paid staff do work that could be done by lower paid staff. The maths doesn’t add up.
Even our IT systems, intended to enable efficiency, often do the opposite. On our consultant WhatsApp group, we joke about “login roulette”: the multiple, complex systems required to complete even the simplest clinical task, which may or may not work on any given day. One colleague recently spent 18 minutes just logging into the systems needed to start a clinic. That’s 18 minutes before any patient care begins. Multiply that across every clinician, every day, and the scale of lost time is enormous.
At the same time, IT teams are understaffed, vacancies remain unfilled, and even straightforward fixes are delayed. Any savings made by reducing digital services are quickly outweighed by the far greater cost of lost clinical productivity, and declining morale across the hospital, every single day.
In oncology, the mismatch between ambition and capacity is particularly stark. NICE approves the majority of cancer drugs it assesses, and once approved, the NHS is legally required to provide them within 90 days. However, while the costs of the drugs themselves are funded, the capacity to deliver them is not. There is rarely additional funding for pharmacists to dispense the drugs, oncologists to prescribe the drugs or scanning capacity to monitor the impact of the drugs. One recently approved breast cancer drug would require an additional 70-90 outpatient appointments every single week. Our clinics are already over-flowing. We can’t simply say yes.
I believe that if we want a functioning system, we must build from the bottom up. Every member of staff should be working at the top of their skillset, not two tiers below it. Instead, we have dismantled the foundation. And things are only getting worse.
We are being asked to save more money. We are being asked to reduce headcount further.
At what point do we stop?
Working in oncology, to a large extent I’m protected from the worst of what is happening elsewhere in the hospital. Stories coming from emergency departments across the country are, frankly, terrifying. Clinicians are trying to provide safe care to tens of patients in corridors, with limited privacy, dignity, and resources. Patients are waiting for hours, sometimes days, on trolleys. The morale injury for patients and staff exposed to these conditions is tangible.
If this is what “it’s about the patients now” looks like in practice, then something has gone very wrong.
There is no simple fix. But for me, continuing to say ‘yes, we can do it’ to NHS England’s demands is not leadership. We can’t simply say yes. The maths does not add up.
In reality, the NHS is already operating in an era of rationing, just not in a transparent or planned way. We ration through delays, workforce gaps, limited access to timely scans, and patients being cared for in corridors rather than beds. It would be better to acknowledge this openly and decide, as we did during the pandemic, what we can and cannot provide, rather than pretend everything is possible and fail by default.
We can’t continue to reduce staff yet simultaneously increase the treatments we aim to deliver. We need to be honest about capacity and be willing to make difficult, explicit choices. That may mean pausing or stepping back from certain services, rebuilding the system from the ground up and only then moving forward in a way that is sustainable.
We can’t continue to just say yes.
The views expressed here are my own and do not necessarily reflect those of the organisations with which I’m affiliated.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}